

Principles in Foot and Ankle Pathology
Which concepts give you the best frame of reference for understanding foot and ankle pathology?
Inversion vs Eversion
Varus vs Valgus
Flat foot vs Cavus Foot
Order of Correction
Muscle Balance
Soft Tissue Management
Rockers
Bony procedures
Osteotomy vs Arthrodesis
Gastrocnemius recesion
1 Inversion vs Eversion (subtalar motion)
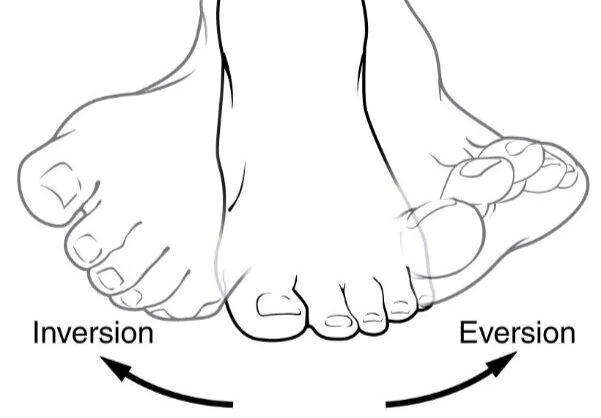
Motion of the subtalar joint
complex 3D movement. It represents the movement of the Talus above the calcaneus and the Midfoot rotating around the head of the talus (Acetabulum Pedis)
2 Varus vs Valgus

Varus and Valgus Hindfoot are asociated with different pathologies, Varus flatfoot is very common and few degrees of varus are badly tolerated. As it locks the subtalar joint in supination and makes a rigid foot that is not able to adapt to irregularities in the terrain
Valgus flatfoot are better tolerated but associated with medial arch colapse
3 Flat foot vs Cavus Foot
PesPlanus are associated with Hallux Valgus, hallux Rigidus, Tibial posterior tendinopathy, sinus tarsi impingment, deltoid ligament and spring ligament ruptures, and subperoneal impingment.
CavoVarus feets (pronated) are associated with rigidity, ankle instability, peroneal tendonitis, lateral ligament sprains, metatarsalgia, claw toes, and dificulty when traversing irregular terrain.
4 Order of Correction
First Correct Hip > Knee > Ankle
Hindfoot > Midfoot > Forefoot
Many of the common problems associated with insatisfaction in patients with otherwise technically correct surgery may be attributed to malalignment of the extremity proximal to the Foot.
Moreover, operating the a complex deformated foot like a Neurologic Cavus varus deformity needs to be planned and operated following the order of PROXIMAL to DISTAL
Correct Equinus deformity
Achilles lengthening
Posterior Capsulotomy
Correct Rearfoot Varus/Valgus
Correct Midfoot Deformity
Abduction / Adduction
Supination / pronation
Correct Forefoot
Flexed or extended first ray
Correct Toes
Claw toes
5 Muscle Balance
There are Muscles that oppose each other, knowledge of the anatomy and function may help in the treatment of some of the conditions
For example in Charcot-Marie-Tooth (CMT) there is an hyperactivation of Peroneus longus (Flexed 1st Ray) and a weak peroneus brevis (loss of eversion)
6 Soft Tissue Management
The foot is a bony structure with little to no fat and soft tissue coverage. The vascularization is really tennous as the majority of the arteries are terminal with little anastomosis.
In our patients there are many risk factors that worsen prognosis such us:
older patients
smokers
diabetics
atherothrombosis disease
Thinking about angiosomes in every approach saves you from one of the most feared complications, wound infection and skin necrosis.

For example in Calcaneus surgery the classic “Lateral L” approach has more wound complications than other locations even when done with the “No touch Technique”
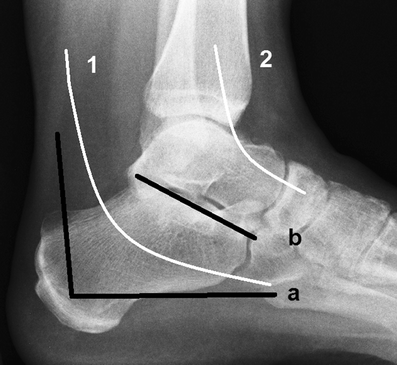
7 Rockers
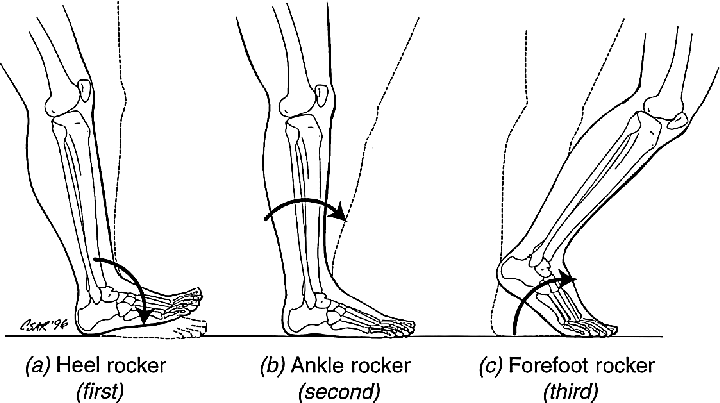
First Rocker doesn’t have Metatarsalgia
Only Talalgia
Second Rocker is associated with Static metatarsalgia
Bony head Height problem
Circular circumscribed callosity
Under the Head
Look in the Lateral Xray or metatarsal view

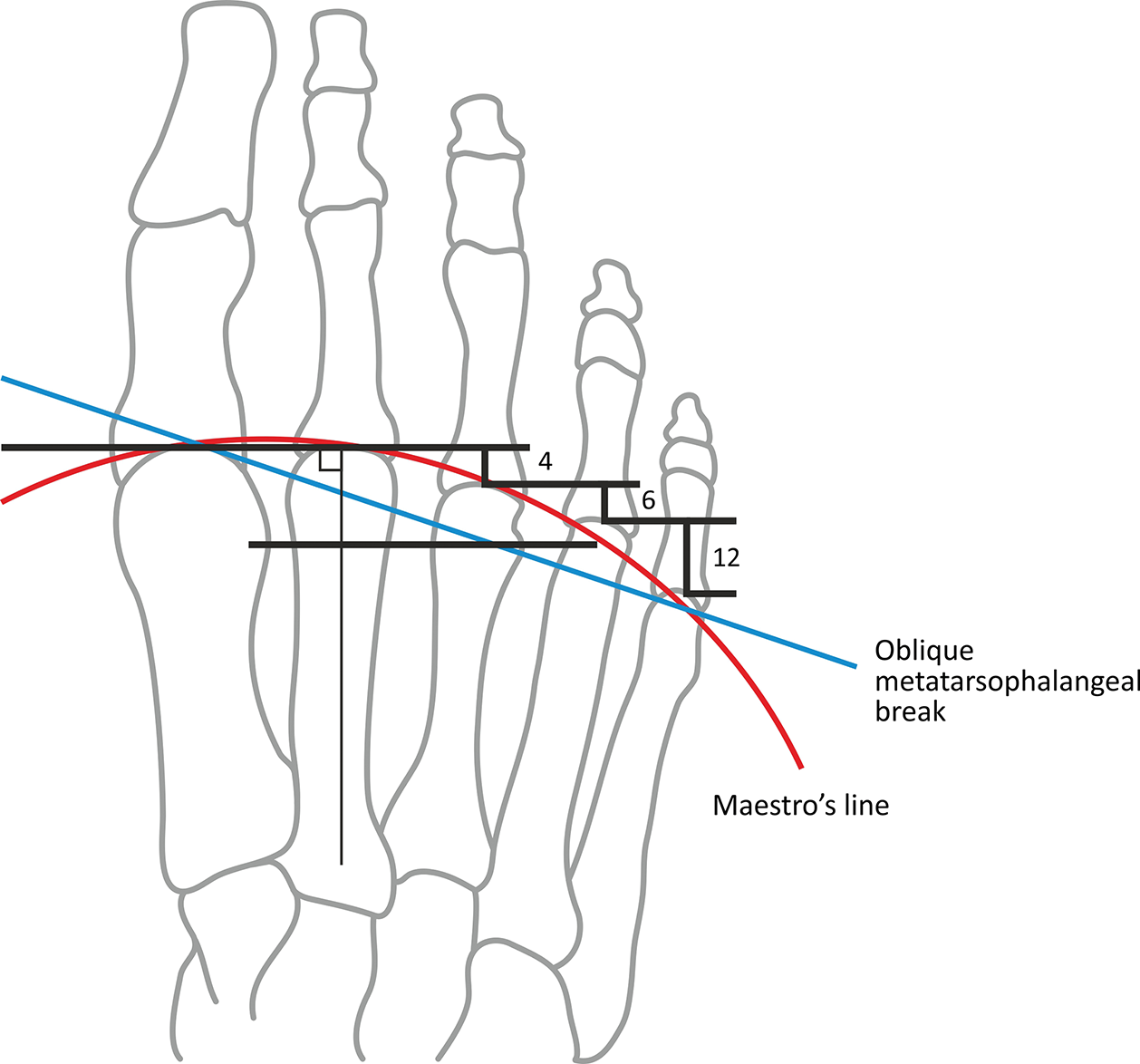
Third Rocker is associated with propulsive metatarsalgia
Bony head length problem
Diffuse callosity
Distal to the head
XRay - weight bearing Dorsoplantar view - Look for Maestro’s Line

8 Bony procedures
In general, most neurologic foot and big deformities need to start with bony procedures because soft tissue procedures alone are not sufficient for correcting deformity and preventing relapses.
9 Osteotomy vs Arthrodesis (fusion)
As a rule of thumb, first you need to catalogue the foot that you are exploring in valgus or varus rearfoot and then you need to assess the mobility and rigidity of the subtalar joint and other neighbour joints. With those two pieces of information you you can decide if osteotomy will be the better treatment (flexible nonrigid non arthritic joint) or fusion (arthritic, rigid foot)
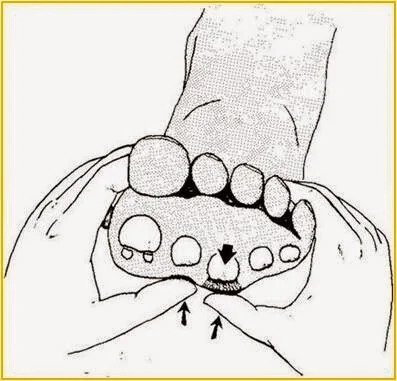
10 Gastrocnemius
Tight Gastrocnemius need to be diagnosed by exploring with the silfverskiold test
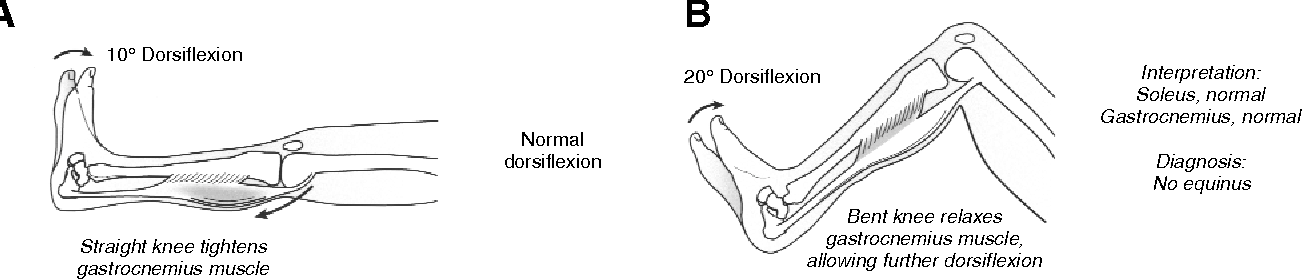
Tight heel cord is associated with equinus foot
It has been published in many articles the relationship between a multitude of foot and ankle pathologies with tight medial gastrocnemius. Doing a proximal lengthening of the medial gastrocnemius is a simple procedure that has great value in improving many conditions.
Eccentric exercise being done daily is associated with improvement in pain and gaining mobility and foot dorsiflexion
Take Home Message
CavoVarus feets (pronated) are associated with rigidity, ankle instability, peroneal tendonitis, lateral ligament sprains, metatarsalgia, claw toes, and dificulty when traversing irregular terrain.
PesPlanus are associated with Hallux Valgus, hallux Rigidus, Tibial posterior tendinopathy, sinus tarsi impingment, deltoid ligament and spring ligament ruptures, and subperoneal impingment.
Read the callosities and Xray of the foot to understand which problem needs to be treated, longitud or height of the metatarsal head.
Bony procedures are the gold standard and soft tissue procedures are done as an associated technique
Rigid and arthritic foot requires fusion for best results
Always look for tight gastroc with silfverskiold test, prescribe eccentric exercise as the first line.
Quitting smoking and getting under control glycemic levels are associated with improvement in the rate of complications after surgery.
Bibliography
Schepers, T. The sinus tarsi approach in displaced intra-articular calcaneal fractures: a systematic review. International Orthopaedics (SICOT)35, 697–703 (2011). https://doi.org/10.1007/s00264-011-1223-9