

Calcaneal Osteotomies. Surgical Tips and Tricks
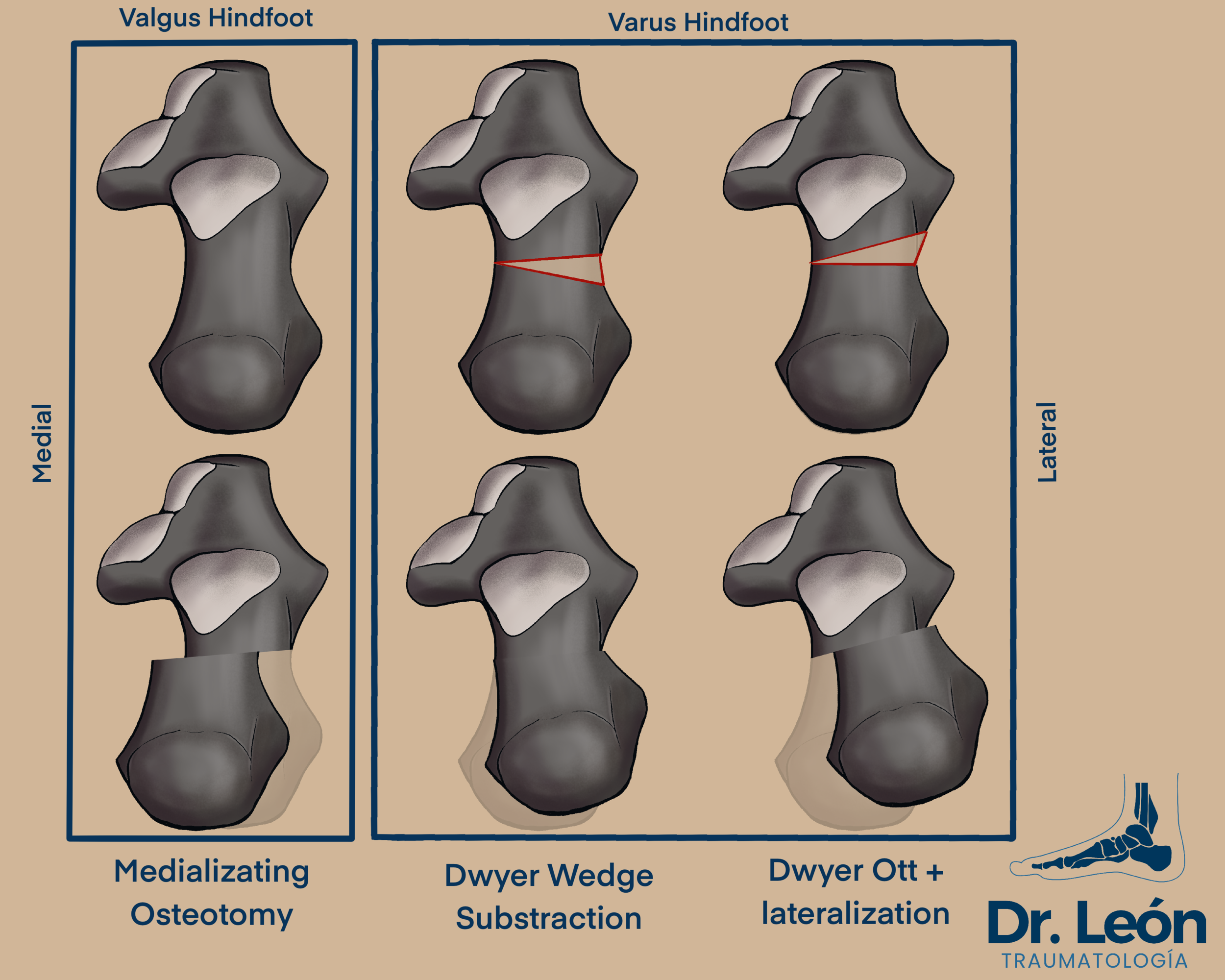
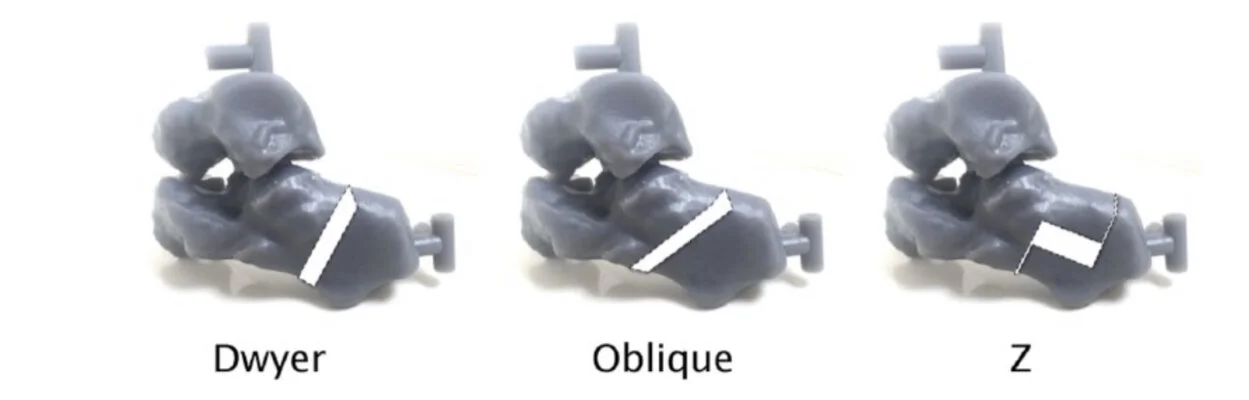
Axial view of three osteotomies
Firs of all, thank you to Dra. Lara Fernández Gutiérrez for helping out with the content of this post. All of the tips and tricks from the percutaneous technique are thanks to her expirience.
This Blog post covers the BASIC osteotomies of the posterior tuberosity of the calcaneus. For Varus foot wedge resection osteotomies and lateralization while for Pes planus medializating sliding osteotomies will be primarely described.
How to do them and tips for easier surgery and new ways to do this classical techniques will also be presented. Also look for links to videos and other techniques.

Osteotomy Principles
Osteotomies of the foot and ankle need to follow the classical advice of “Measure Twice and Cut Once”.
Osteotomies are complex 3D Cuts that change the anatomy and biomechanics with little variation of hand placement or saw inclination.
Careful planning, knowledge of the relevant anatomy and visualization of the planes of cut will lead to the best results.
So slow down before cutting, take your time and cut once, to be the fastest on the Operating Room.
Calcaneal osteotomies present in many flavours, which to choose and how to do it effectively?
Koutsogiannis vs Dwyer osteotomy?
Koutsogiannis described an osteotomy based on medial sliding displacement of the posterior tuberosity of the calcaneus
Koutsogiannis is usually indicated in a valgus rearfoot (flat foot) to medialize the posterior tuberosity and create biomechanical advantage for the achilles tendon.
Medializing the posterior tuberosity also improves subtalar joint biomechanics by impeding over pronation of the subtalar joint in the second rocker.
It also improves static by alleviating medial soft tissue tension and overuse of posterior tibial tendon.
Dwyer osteotomy - More distal osteotomy = lesser lever arm = less correction
Dwyer osteotomy - proximal osteotomy, longer lever arm. More correction
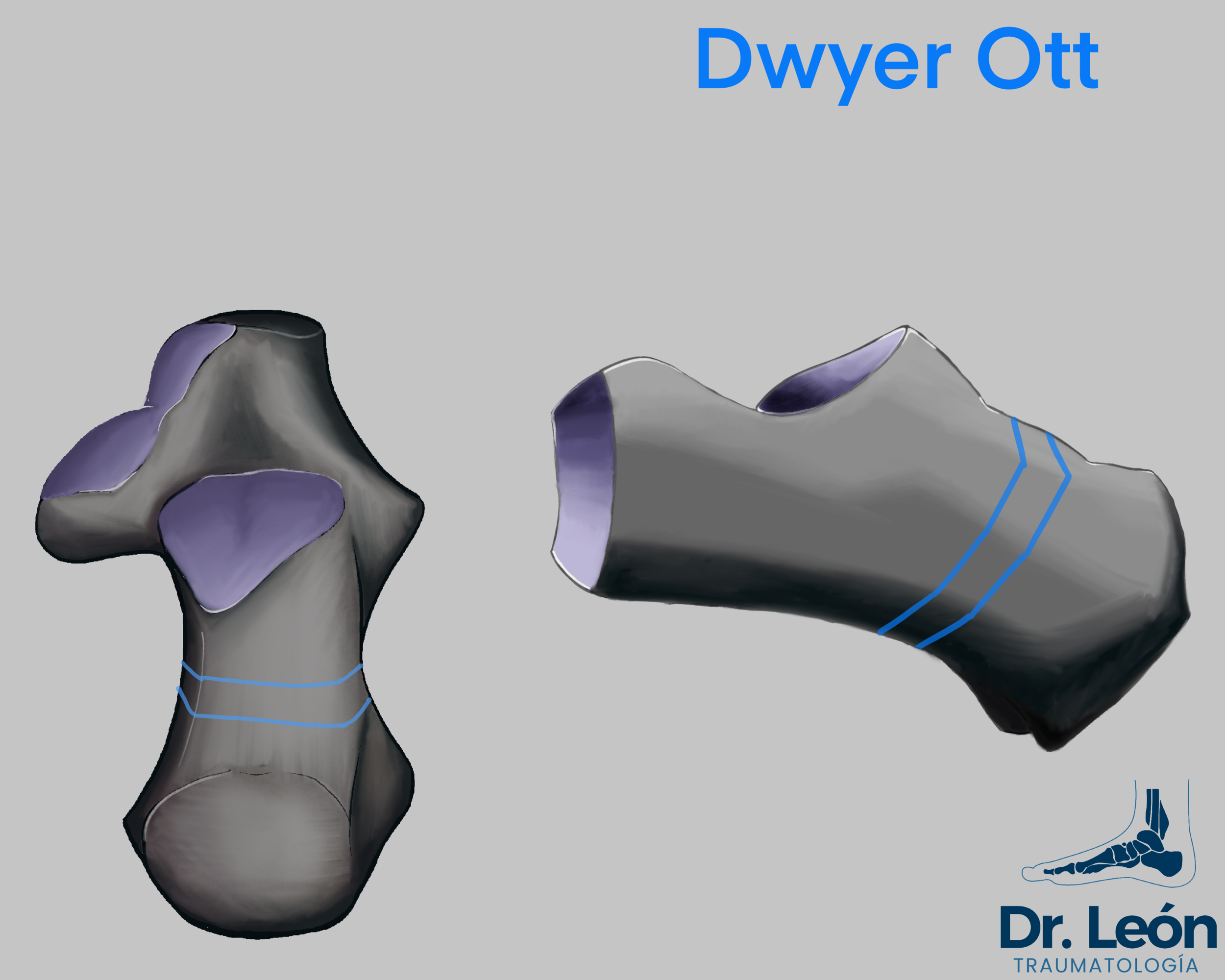
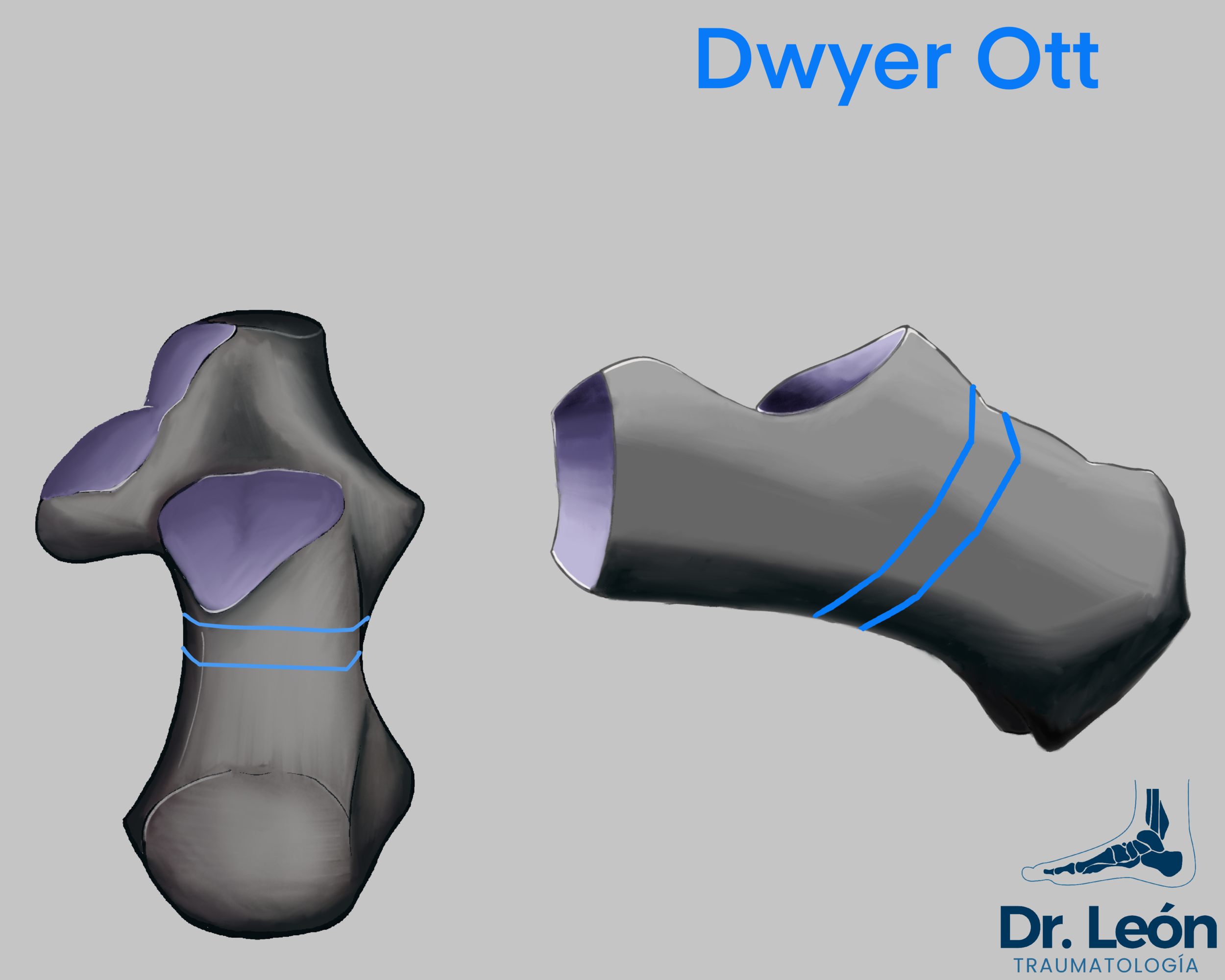
Dwyer osteotomy is made by subtracting a lateral-base wedge from the calcaneal wall.
It is usually indicated in Varus rearfoot. Calcaneus varus usually has some degree of internal concave curve to its body, in contrast to flatfoot that the calcaneus is straight.
By subtracting a 1cm base lateral wedge, the axis of the calcaneus becomes straighter.
If the displacement is not enough it can be associated with a lateral slide of the posterior tuberosity (1cm displacement).
Closing wedges of the calcaneus and lateral displacement leads to “unlocking” the subtalar joint, giving it a chance to pronate and adapt to irregular terrain.
It also improves lateral tightness and tension of the peroneal tendons and lateral ligament complex of the ankle.

Zadek Osteotomy, Dorsal Wedge used to treat achilles tendinopathy
Reverse Koutsogiannis is also known as a lateral sliding displacement of the posterior tuberosity.
Not routinely done as a stand alone procedure because the calcaneus has a C shape curvature of the body as explained previously
Can be indicated at the same time as dwyer osteotomy
Zadek osteotomy, subtracts a dorsal base wedge in achilles insertional tendinopathy.
The biggest downside is the loss of the lever arm for the achilles tendon.
But, Is there anything new? - Presenting the Z osteotomy
Z osteotomy was designed to simplify 2 osteotomies of the calcaneal flatfoot into one single approach.
Medializing osteotomy for the posterior tuberosity
Lateral column lengthening
It has been shown in 3D printed studies to be better than dwyer ott in managing greater deformities, It can rotate the Posterior tuberosity in the coronal plane, but has not been compared to the Dwyer + lateralizating procedure
It is more complex than other osteotomies and needs further investigation to describe where and how long to make the osteotomies.
For flatfoot reconstruction Tantalum wedges can be placed to gain longitud
The approach is also larger and needs to be gentler to not damage the peroneal tendons or the sural nerve.
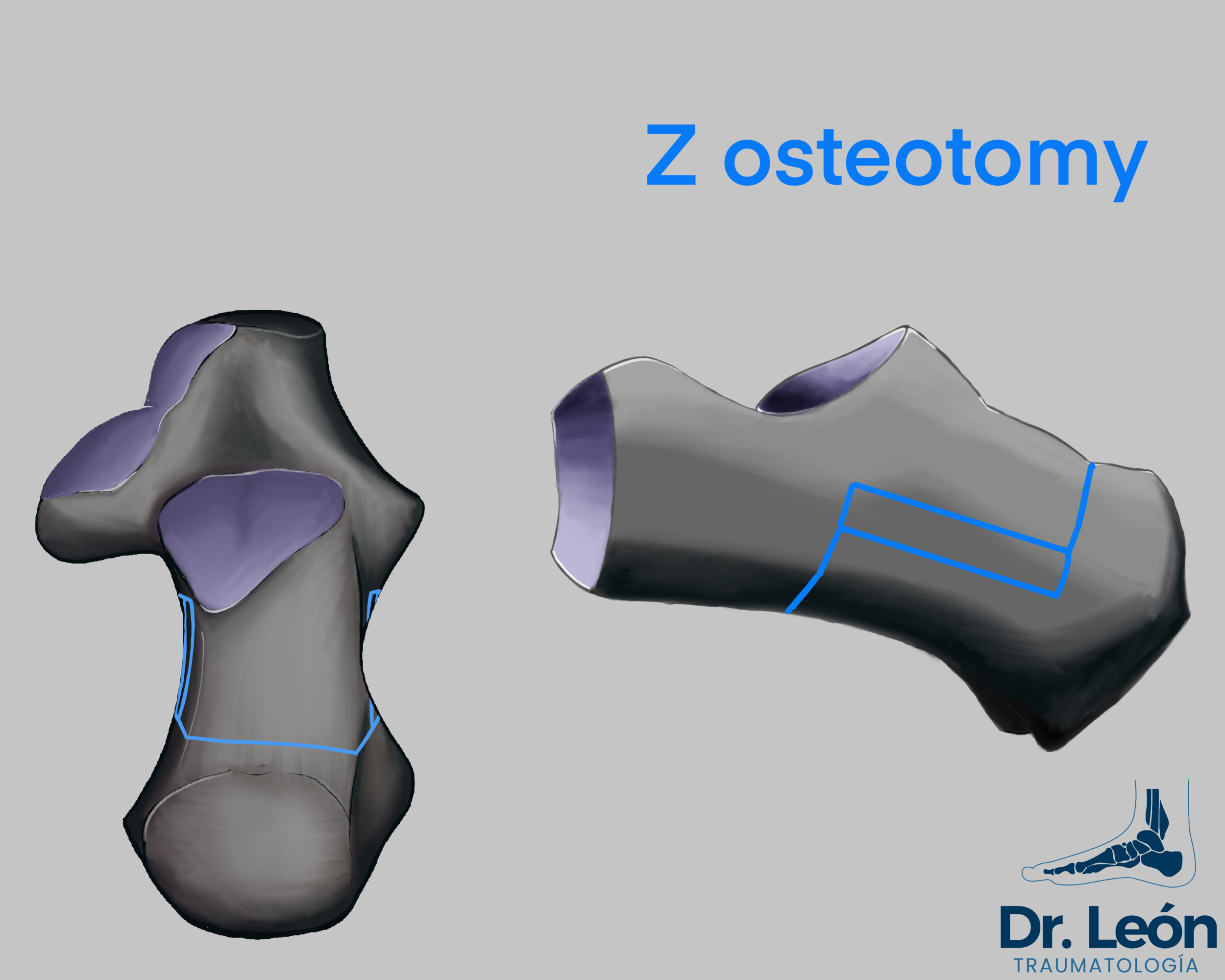
Z osteotomy, inspired by scarf osteotomy of M1 can be made to correct complex deformities of the calcaneus with a single approach
Z Osteotomy. Using a needle to plan for the horizontal osteotomy. tantalum wedges to create medial displacement and lateral column lengthening (Evans effect)
What are some Technical Tips for better results?

5 min automatic retractor.
Using a laminar spreader or similar automatic distractor. Placed in the osteotomy for 5 min to make the medial soft tissues to loosen up some tension.
It can help with medial periosteum that limits translation.
Especially indicated in varus foot, before closing and lateralizing the osteotomy.
Waiting for 5 min looks like a waste of time, but combined with plantar flexion it frees the posterior tuberosity to be moved and saves time in the long run.

Wide Lambotte bone chisel
Used as a reference for the position of the osteotomy. Place the wide chisel as a line and take some xrays to see if the position is appropriate or needs to be changed.
Mark the line impacting it with a hammer.
When the osteotomy is finished, place two lambotte wide bone chisels inside the osteotomy and use the hammer in the middle as a fulcrum to make a lever and open the space for the bone to move.
The always present K wire may also be used for the purpose of marking the osteotmy
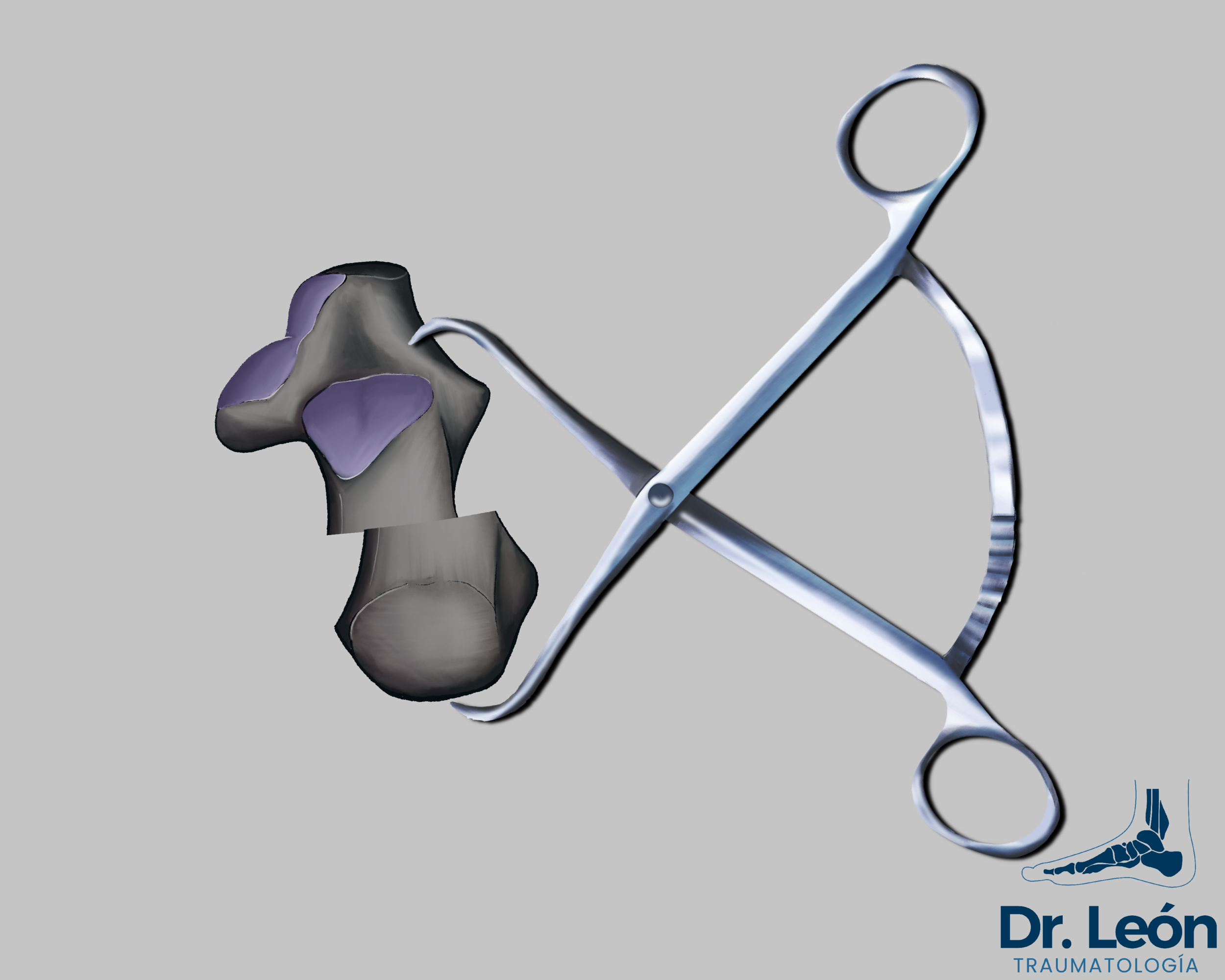
Codevilla bone forceps used to maintain reduction
The use of two K wires and a ruler while viewing in an axial (Harris) view can make it easier to incline the osteotomies to make a perfect triangle wedge, following the direction that you want
It can also be used to mark the osteotomy. Place it inside the approach, flat on top of the lateral wall and take some x rays.
Use a “Codevila bone reposition forceps” to maintain reduction.
Place one of the arms of the forceps in the lateral aspect of the tarsal tunnel above the anterior apofisis of the calcaneus
Place the other arm on the posterior aspect of the calcaneus
This maneuver frees the surgeon hands to move the ankle and take some x rays while placing provisional K wires.
What is MICO all about?
MICO (Minimally invasive calcaneal osteotomy) - Percutaneous osteotomy of the Calcaneus, is made with high speed burr and fluoroscopic imaging
V osteotomy (CHEVRON) vs Straight (in biomechanical model, V osteotomy was better regarding cicles of load to failure)
Percutaneous calcaneal osteotomy is a novel technique especially indicated in those patients with previous pathology (Diabetes Mellitus, vasculopathy…) who may have healing problems and in those who have soft tissue injuries and previous scars.
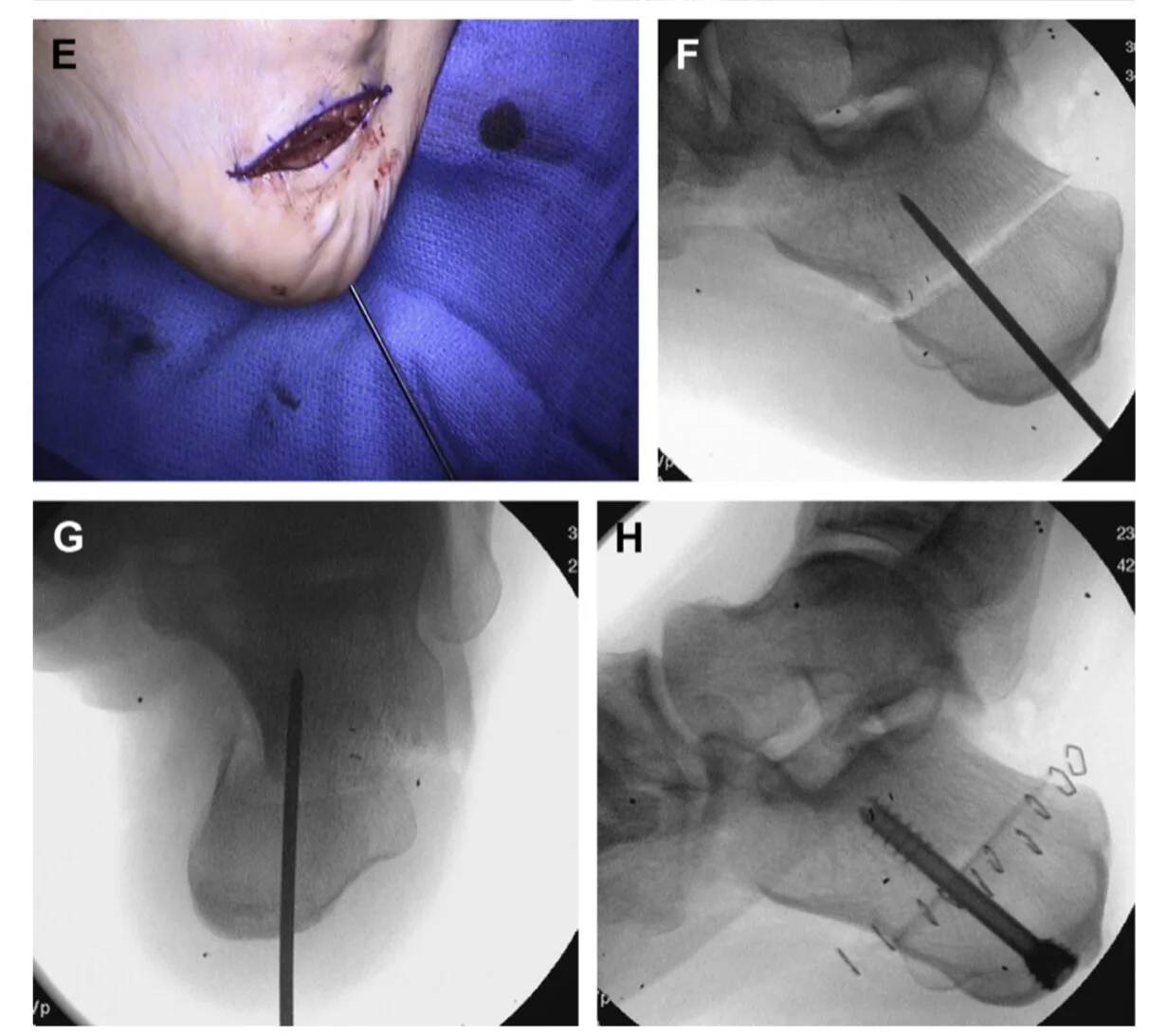
Surgical technique
Place the patient in lateral decubitus with a support in the pubis and another in the gluteus and a pillow between both lower extremities, the contralateral lower extremity will be bent so that it does not overlap on the radiograph. Although it is a technique that does not require ischemia, we will place the ischemia cuff because we will frequently associate other surgical gestures.

MICO (Minimally invasive calcaneal osteotomy)- safe zone represented in red.
The fluoroscope will be placed on the patient's back and with the fluoroscopy assistance we will draw the osteotomy taking into account the anatomy and especially the branches of the sural nerve, for this we will have a safety corridor about 11mm ahead of the line that runs from posterior tuberosity to fascia lata insertion (Talusan et all).
We start at the apex of our Chevron-type osteotomy, crossing both cortical bones.
We will perform a V osteotomy with two lines inclined about 15-30º forward with respect to the perpendicular to the long axis of the calcaneus, in the following order:
1st. Dorsal.
2nd. Plantar
Try not to exceed 6000rpm and maintain a continuous irrigation with saline solution to avoid thermal necrosis.
We check that the osteotomy is complete by freely moving the calcaneal tuberosity. Through the incision we introduce a periosteal elevator that will allow us to mobilize the osteotomy, the correction will be verified with an axial projection.
It is advisable to keep the knee flexed to prevent the Achilles from preventing the desired correction.
After achieving the appropriate correction, we will place two K-wires on which we will place two cannulated 5.5-7mm diameter compression screws.
What are the most common errors to avoid?
Leaving serrated borders
Being careful with the osteotomy cut and moving the oscillating saw in the same plane will make straight borders.
Changing planes and tilting the oscillating saw or moving the foot will make serrated borders that bite into each other and limit the medio-lateral displacement of the osteotomy.
Step off
When the Osteotomy is made and fixed there is a step off remaining on the lateral side.
To fix the sharp edges and remove any protruding bone that may irritate the lateral soft tissues, use a bone graft impactor. This tip is usually more challenging than expected and making some perpendicular chisel
Elevation and shortening of the lever arm
Calcaneal osteotomies, especially in tight soft tissue foot (Cavo varus) tend to follow the path of less resistance and move Up and shorten.
Following the principles described previously to lengthen soft tissues for 5 min help alleviate this problem
Also being mindful of how to make the Dwyer osteotomy in the axial plane can help with avoiding shortening (Imagen)
Not doing the osteotomy in the desired place
it’s associated with skipping the step of taking xrays. There are multiple techniques
Kwire superpose with calcaneus + xray
Osteotome
K wire pinned as reference
Reese guide
Overpenetration or overheating
Do the osteotomy in two steps, lateral wall first and then medial (Finish with osteotome)
Careful with blunt saw, use saline to prevent overheating of the bone and thermal damage
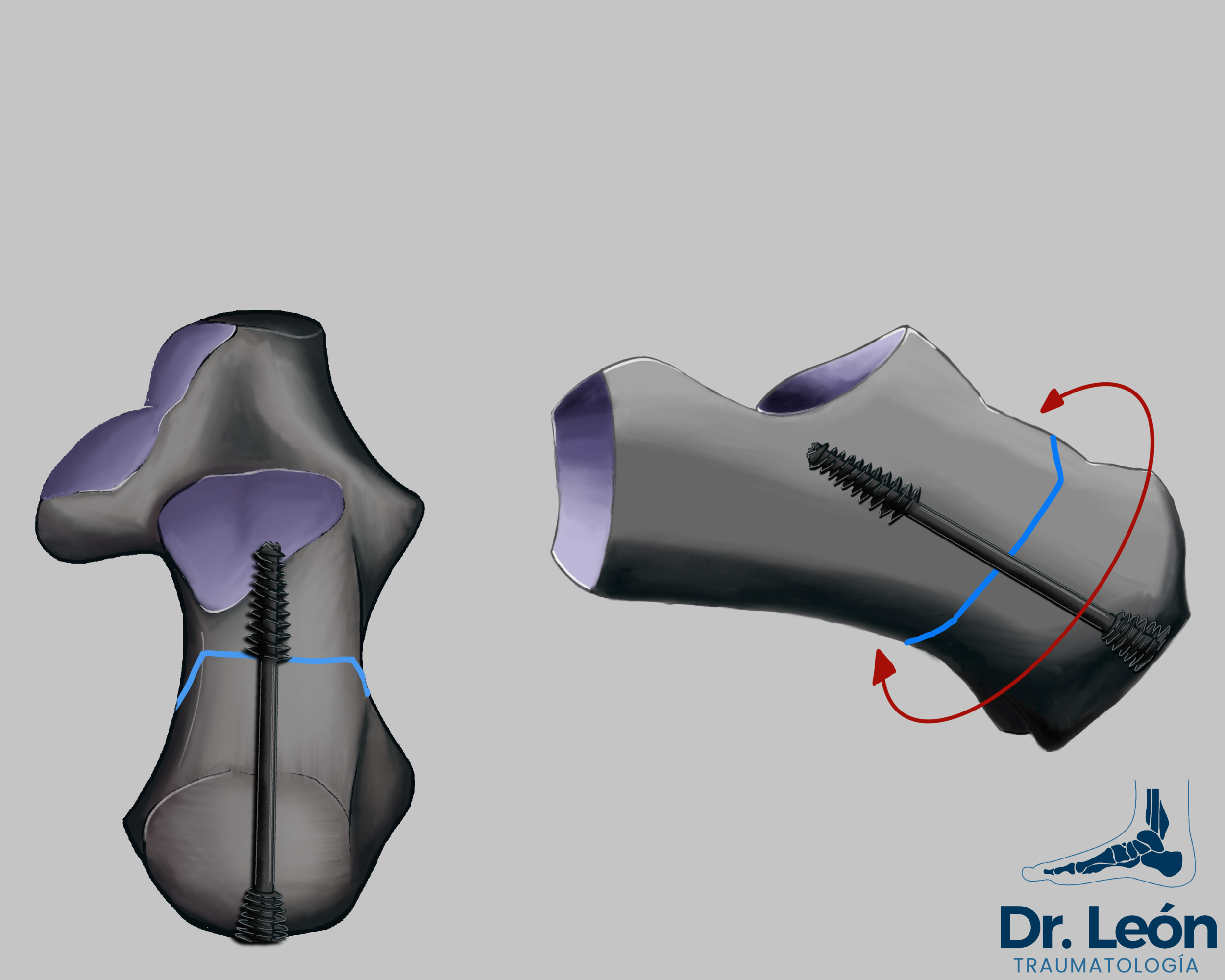
Screws need to be centered
on the calcaneal tuberosity to penetrate both parts of the bone and need to be perpendicular to the osteotomy.
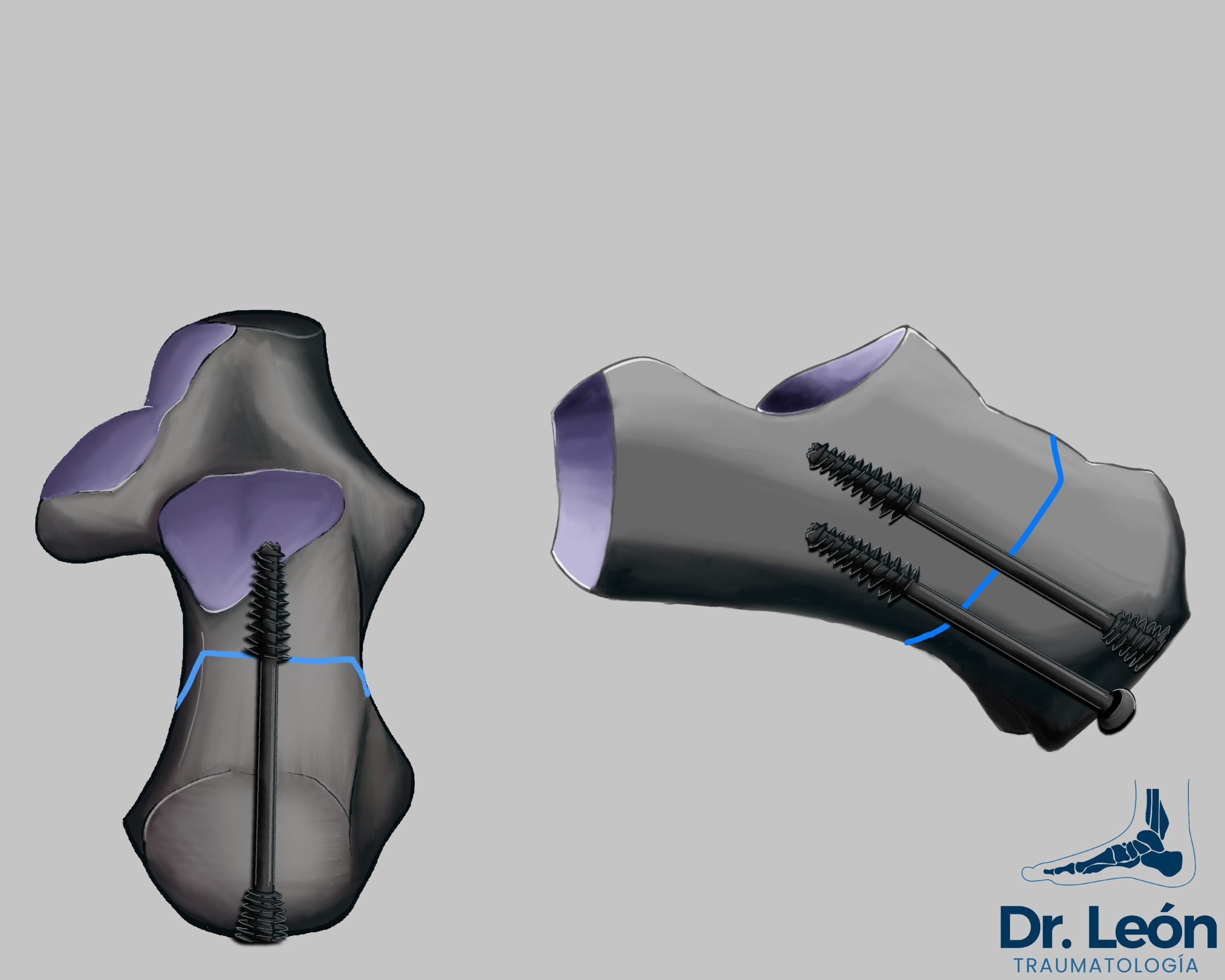
1 screw is theoretical possible but two may prevent rotation in the coronal plane.
Failure to close the wedge osteotomy
even helped with dorsiflexion of the foot may be related to a bone wedged in between the osteotomy site.
Synthesis
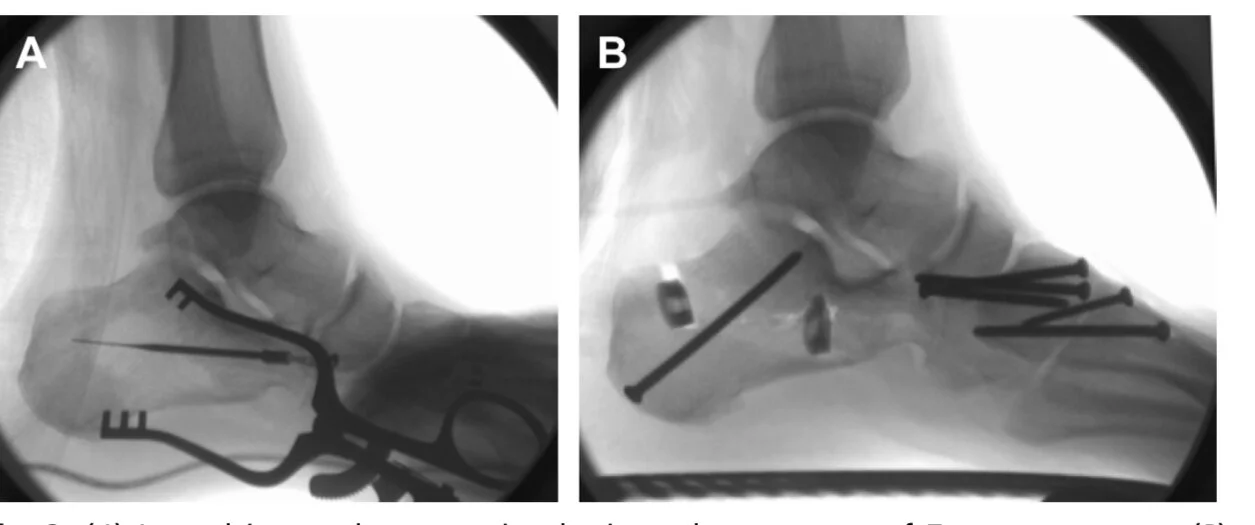
Take a look at the headless screw vs the head screw. The latter may cause pain and discomfort.
Clinical case representing medializating osteotomy
Plates are made with step off in mind
Usually are more expensive.
They are presented with a variety of stepoff options and offset to facilitate reduction. They can be even placed inside the proximal calcaneus to reduce the profile.
Cannulated partial screws
No-head screw has shown to be associated with less pain in the talar region.
x2 screws are better than one to prevent rotation in the coronal plane and minimize shearing forces. Patients can begin weight bearing earlier with this construct
Staple is another option, need to have a stepdown premade to have lesser profile and lower the risk of irritation of the skin
Usually recomended in pediatric population to decrease the risk of damagin the physis
x2 k wires have been described, the synthesis is the cheapest of the above but it is associated with more time to heal with no weight bearing and risk of superficial pin infection.
How much to displace?
1CM RULE
The rule is 1cm for medial displacement (Steffensmeier SJ et all)
For Dwyer 1cm base wedge (for mild deformity) + 1 cm lateral slide if (moderate to severe deformity)
Once Operated, how is the postoperative management?
This procedure needs protected weight bearing until bony union. One way to treat this patients can be:

First 2 weeks splint bellow the knee. Then transition to
Cast boot
Walker boot
Begin moving Tibiotalar at 4w
Nonweight bearing 6w or until xray signs of consolidation.
Beware that Diabetic of smokers may need more time until weight bearing is allowed.
If pain in the osteotomy site, be careful with transitioning to WB.
Maintain Walker boot until 10 to 12 weeks, wound closed, no pain on osteotomy, xray signs of bone healing
Take Home Message
Varus foot are associated with “C shape body” of the Calcaneus, It needs to be corrected by closing wedge osteotomy (Dwyer)
Valgus foot collapse under the weight of the body, The calcaneus is straight, it only needs to be moved under the mechanical axis of the leg.
Techniques are not excedingling complex but results can vary between knowing the best practices to avoid complications. There are many paths to a successful surgery, knowing different techniques and surgical tips could mean the painless solution of an unforeseen problem.
Osteotomies of the calcaneus have been known for decades and the results have been proven effective. But consider them a part of a whole arsenal of techniques, ranging from osteotomies to soft tissue techniques.
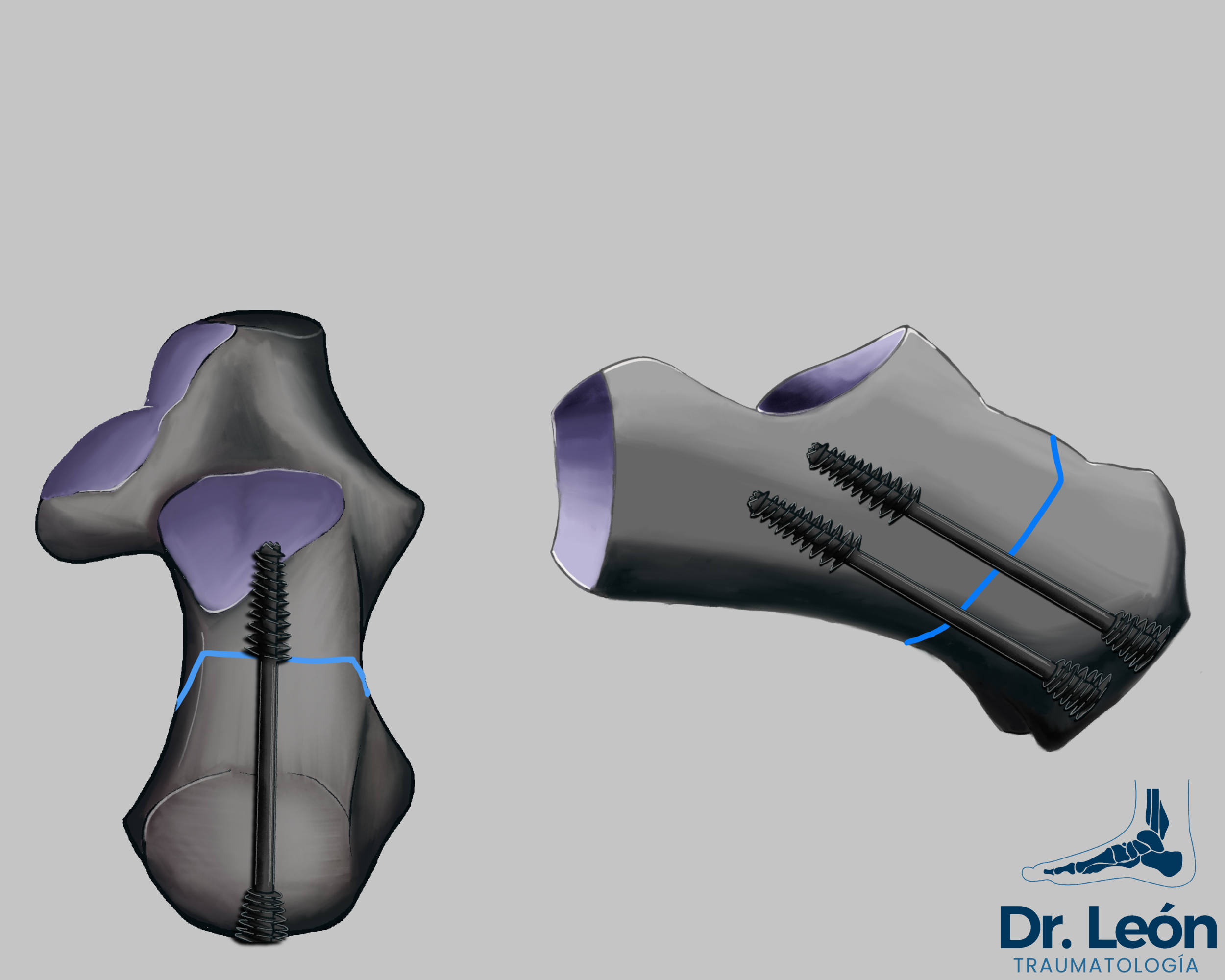
Proposed fixation for osteotomy
Original article osteotomy of the calcaneus
Bibliography
Greenfield S, Cohen B. Calcaneal Osteotomies: Pearls and Pitfalls. Foot Ankle Clin. 2017 Sep;22(3):563-571. doi: 10.1016/j.fcl.2017.04.011. Epub 2017 Jun 9. PMID: 28779807.
MDCO - Medializing calcaneal Osteotomy for adult acquired flatfoot review of technique
Vienne P, Schöniger R, Helmy N, Espinosa N. Hindfoot instability in cavovarus deformity: static and dynamic balancing. Foot Ankle Int. 2007 Jan;28(1):96-102. doi: 10.3113/FAI.2007.0018. PMID: 17257547.
Shim DW, Suh JW, Park KH, Lee JW, Byun J, Han SH. Diagnosis and Operation Results for Chronic Lateral Ankle Instability with Subtle Cavovarus Deformity and a Peek-A-Boo Heel Sign. Yonsei Med J. 2020 Jul;61(7):635-639. doi: 10.3349/ymj.2020.61.7.635. PMID: 32608208; PMCID: PMC7329740.
Durston A, Bahoo R, Kadambande S, Hariharan K, Mason L. Minimally Invasive Calcaneal Osteotomy: Does the Shannon Burr Endanger the Neurovascular Structures? A Cadaveric Study. J Foot Ankle Surg. 2015 Nov-Dec;54(6):1062-6. doi: 10.1053/j.jfas.2015.05.007. Epub 2015 Jul 23. PMID: 26210080.
2 consultants and 11 inexperienced surgeons performing MICO surgery on cadaver.
No mayor NV lesions, only 2 secondary branches of sural nerve damaged
Safe approach
Gutteck N, Haase K, Kielstein H, Delank KS, Arnold C. Biomechanical results of percutaneous calcaneal osteotomy using two different osteotomy designs. Foot Ankle Surg. 2020 Jul;26(5):551-555. doi: 10.1016/j.fas.2019.07.004. Epub 2019 Jul 22. PMID: 31371267.
V osteotomy better than straight (Load cicles to failure)
Ebaugh MP, Larson DR, Reb CW, Berlet GC. Outcomes of the Extended Z-Cut Osteotomy for Correction of Adult Acquired Flatfoot Deformity. Foot Ankle Int. 2019 Aug;40(8):914-922. doi: 10.1177/1071100719847662. Epub 2019 May 14. PMID: 31088118.
Z osteotomy with wedge addition to simplify two calcaneal osteotomies
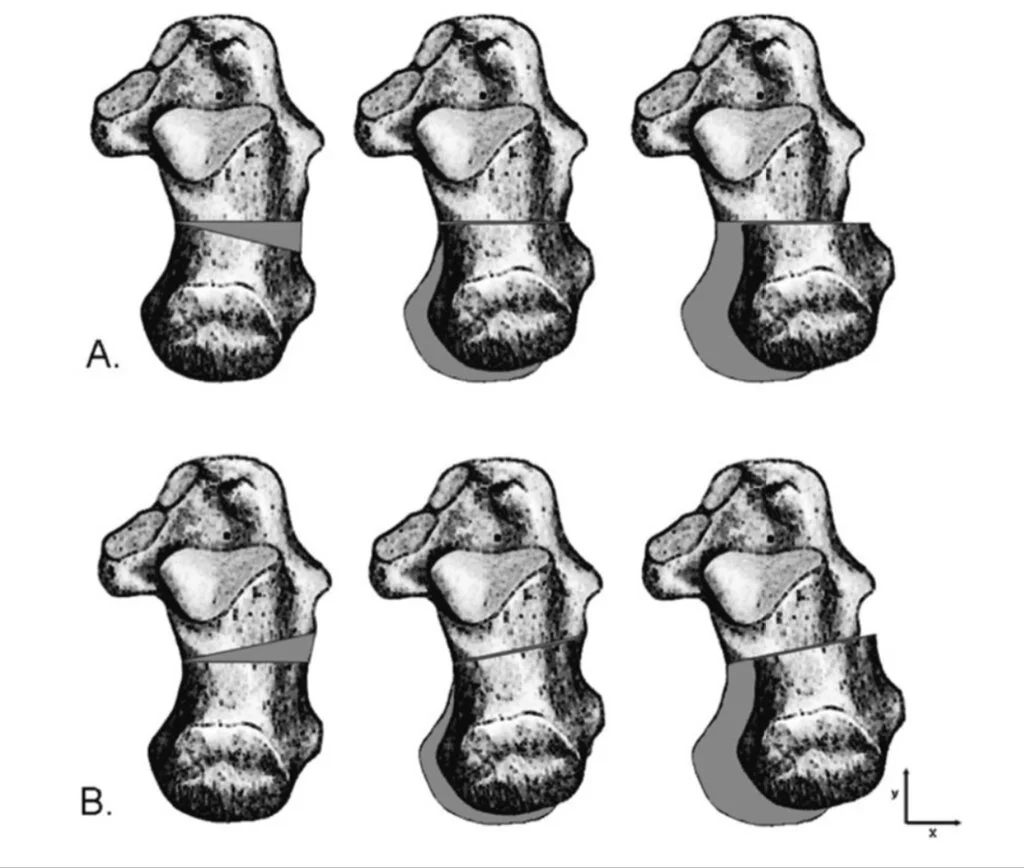
Kraus JC, Fischer MT, McCormick JJ, Klein SE, Johnson JE. Geometry of the lateral sliding, closing wedge calcaneal osteotomy: review of the two methods and technical tip to minimize shortening. Foot Ankle Int. 2014 Mar;35(3):238-42. doi: 10.1177/1071100713518188. Epub 2013 Dec 26. PMID: 24371022.
Osteotomies of the calcaneus - Different angles
Shortening and translation
Ott usually shortens lenght of lever
Proposed change of cut angulation to get more correction
Jaffe D, Vier D, Kane J, Kozanek M, Royer C. Rate of Neurologic Injury Following Lateralizing Calcaneal Osteotomy Performed Through a Medial Approach. Foot Ankle Int. 2017 Dec;38(12):1367-1373. doi: 10.1177/1071100717728678. Epub 2017 Sep 1. PMID: 28863729.
It is safe to approach from the medial side. No more risk of tarsal tunnel syndrome
Scott RT, Berlet GC. Calcaneal Z osteotomy for extra-articular correction of hindfoot valgus. J Foot Ankle Surg. 2013 May-Jun;52(3):406-8. doi: 10.1053/j.jfas.2013.01.005. Epub 2013 Feb 28. PMID: 23453608.
Combining of posterior and lateral column lengthening osteotomies
Pes planus correction
Complex technique, 1 incision
Feuerstein CA, Weil L Jr, Weil LS Sr, Klein EE, Agerakis NG, Akram U. The calcaneal scarf osteotomy: surgical correction of the adult acquired flatfoot deformity and radiographic results. Foot Ankle Spec. 2013 Oct;6(5):367-71. doi: 10.1177/1938640013499627. Epub 2013 Aug 21. PMID: 23966258.
Scarf Technique retrospective study
Very detailed technique and results
Possible to make needed corrections with good results
Pfeffer GB, Michalski MP, Basak T, Giaconi JC. Use of 3D Prints to Compare the Efficacy of Three Different Calcaneal Osteotomies for the Correction of Heel Varus. Foot Ankle Int. 2018 May;39(5):591-597. doi: 10.1177/1071100717753622. Epub 2018 Jan 24. PMID: 29366341.
Dwyer vs Oblique vs Z osteotomy wedge resection
No lateral displacement of any ott, need associated procedures
3d model
Dwyer and oblique risk of shortening. For mild deformity best
Z osteotomy corrects coronal plane deformity but not lateralization (only rotation)
Talusan PG, Cata E, Tan EW, Parks BG, Guyton GP. Safe Zone for Neural Structures in Medial Displacement Calcaneal Osteotomy: A Cadaveric and Radiographic Investigation. Foot Ankle Int. 2015 Dec;36(12):1493-8. doi: 10.1177/1071100715595696. Epub 2015 Jul 31. PMID: 26231200.
safe zone as an area on the lateral foot radiograph extending 11.2 mm anterior from a line connecting the posterior superior apex of the calcaneal tuberosity to the origin of the plantar fascia
Wills B, Lee SR, Hudson PW, SahraNavard B, de Cesar Netto C, Naranje S, Shah A. Calcaneal Osteotomy Safe Zone to Prevent Neurological Damage: Fact or Fiction? Foot Ankle Spec. 2019 Feb;12(1):34-38. doi: 10.1177/1938640018762556. Epub 2018 Mar 13. PMID: 29532743.
No more risk by doing osteotomy proximal to “safe zone”
Steffensmeier SJ, Berbaum KS, Brown TD, et al. Effects of medial and lateral displacement calcaneal osteotomies on tibiotalar joint contact stresses. J Orthop Res 1996;14(6):980–5.
1cm displacement medial osteotomy changes in contact pressure
Boffeli TJ, Abben KW. Double calcaneal osteotomy with percutaneous Steinmann pin fixation as part of treatment for flexible flatfoot deformity: a review of consecutive cases highlighting our experience with pin fixation. J Foot Ankle Surg. 2015 May-Jun;54(3):478-82. doi: 10.1053/j.jfas.2014.04.017. Epub 2014 May 21. PMID: 24856664.
2 k wires synthesis
Pfeffer GB, Michalski MP, Basak T, Giaconi JC. Use of 3D Prints to Compare the Efficacy of Three Different Calcaneal Osteotomies for the Correction of Heel Varus.
Most of the Images in this Blog are made by me with Procreate 5 for the Ipad. The rest are taken from the Google Images. Last Edit or update of this Post: 03/08/2021
If what you have read it’s of your liking take a look at other post and follow on social media for new content and updates in orthopaedic surgery.